Dom Cooper looks at serious injuries and fatalities (SIF) in the workplace, analysing whether the current OSH approach is working and what the resolution may be instead.
Introduction
Over the past few years, I have spent considerable time pondering why serious injuries and fatalities (SIFs) keep rising in the workplace. According to the International Labour Organisation (ILO), there were an estimated 1 million SIFs in 1999 and 2.78 million in 2017[i]. It is a global problem overly represented in agriculture, construction, forestry, fishing & hunting, manufacturing, mining and transportation & warehousing.
Those most at-risk are temporary, casual or part-time workers in small and medium enterprises. A joint World Health Organisation (WHO) and ILO study suggests the occupational risk factors with the largest number of attributable deaths was [1] ischaemic heart diseases from long working hours (55 hrs+ p.w.), followed by [2] exposure to COPD from occupational particulate matter, gases and fumes, and [3] occupational injuries[ii]. The ILO says the common reasons are [a] deficiencies in national OSH systems, including the legislative framework; [b] weak regulatory oversight; and [c] the absence of a culture of safety and health at the national and workplace levels. The impact of economic cycles could also be at play[iii].
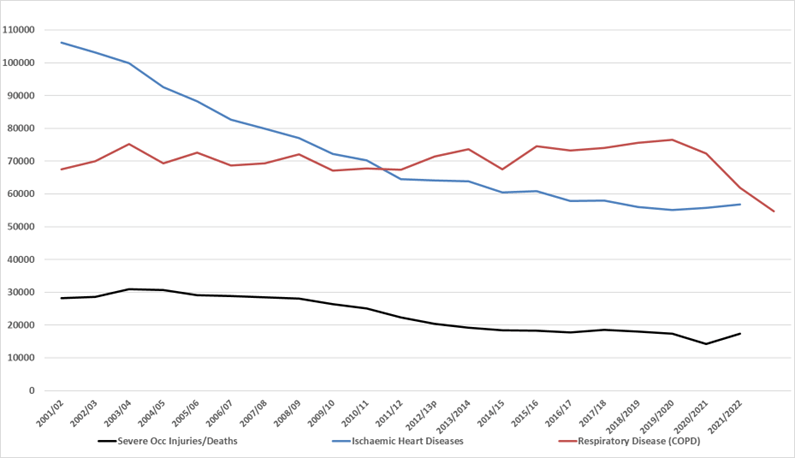
Using the past 20 years’ UK RIDDOR and English & Welsh coroners’ records, figure 1 is indicative of the extent of SIFs in Britain. While work-related ischaemic heart disease deaths have reduced, the data largely indicate that British SIF reduction has plateaued over the past decade.

Figure 1: A picture of Britain’s SIF problems from 2001-2022
Current OSH Approaches
This past year or so, I have studied various OSH remediation approaches being heavily promoted to the profession. Published by SHP, these include:
- New View Safety, whose ideology is not sufficient to prevent harm. OSH requires structured and consistent approaches to be successful;
- Mental Health self-report incidents are far greater than actual clinicians’ reports. Mental health cases are much less of a UK problem than minor illnesses, musculoskeletal problems or accidents;
- High-Reliability Organisations’ are unclear on the links between HRO principles and performance, but the basics of standard safety management are vital to actual improvements;
- Psychological Safety exerts an inconsistent impact on error reporting (showing that association is not causal); tangible situational safety factors exert a much greater influence;
- Just Cultures don’t lead to increased reporting of incidents or errors, and blame for incident involvement depends on intention;
- Trust, mistrust or distrust lead to a complex pattern of positive and negative outcomes, suggesting the importance of understanding how an entity is fostering trust, mistrust and distrust [a] in its approach to safety, [b] among its personnel, and [c] in its systems, equipment, processes and procedures;
- Wellbeing interventions don’t work with either an individual or organisational focus, or reduce injuries. Conversely, reducing SIFs improves workplace wellbeing;
- Aggregated lost-time and total-recordable Incident Rates are unreliable and are therefore invalid as meaningful measures of safety performance.
Relationships between current OSH Approaches and SIFs
Taking a detached view of these current OSH approaches reveals the OSH profession has latterly been, and is, overly concerned with the psychological aspects of OSH (i.e., mental health, psychological safety, just cultures, trust and wellbeing) rather than people’s physical safety. In terms of OSH management, new-view safety paradigms of high reliability and resilience engineering have tended to dominate the OSH airwaves of late, despite there being no evidence that they lead to incident reduction[iv].
Epiphenomena
Of fundamental importance is that all the above approaches are ‘epiphenomena’: i.e., they are incidental secondary effects or byproducts that arise from, but do not causally influence their primary process as they have no effects on their own.
For example, wellbeing and mental health are subjective states largely determined by our personality and perceptions of people, circumstances or events that impact upon us. Psychological safety and a (un)just cultures are both something done to us and, therefore, entirely out of our control.
Similarly, trust, mistrust and distrust are dependent upon entities, people or objects meeting our expectations. Since epiphenomena doesn’t have any causal influence on the primary phenomenon, they are very unlikely to have predictive value. This means reliability, resilience, mental health, psychological safety, justness, trust and wellbeing do not, and will not, causally predict or prevent SIFs, or indeed those things they are intended to fix (e.g., error reporting), as the research on current approaches above has shown. In turn, if the global SIF problem is to be reduced, this means it is imperative the global OSH profession return its focus to those approaches known to reduce physical injuries.
Known Approaches that Reduce SIFs
A culture of safety or ‘safety culture’, as it is commonly termed, has been linked to incidents and incident reduction[v]. Based on research, it behoves entities to create & support an atmosphere of high risk-aversion & low risk-tolerance; focus on putting safety before profit via a ‘safe-production’ ethos; eliminate any culture of fear; uplift the safety knowledge and authority of leaders, buttressed by holding them responsible and accountable for OSH; ensure managerial compliance with OSH rules & procedures; improve two-way safety communications; increase personnel’s cognitive, functional and enabling competencies; and improve any lessons-learned processes, including the corrective and preventive action element. Periodic diagnostic cultural assessments can also assist greatly.
Formal evidence-based behavioural based safety processes, implemented correctly, have a 40-year-plus track record of reducing injuries and are ideally suited to tackling the SIF problem[vi]. Trained workgroup-based observers who actively monitor their colleagues’ behaviour and their working environment are able to spot situations in which someone is at great risk of being hurt and intervene before that risk comes to fruition[vii]. Similarly, workgroup-based initiatives that seek out and fix situations that are human error traps (things that induce human error) can also exert a dramatic effect[viii]. However, both behavioural and human error approaches must be maintained for a number of years, or else their effect can rapidly decline.
High-quality safety management systems and standards can also help enormously[ix], but they must not become the bureaucratic be-all and end-all of safety. A genuine safety partnership between leadership and employees engaging people in the safety effort is the key to unlocking the SIF problem. Similarly, monitoring progress by using leading performance indicators that focus on the processes that lead to the desired outcomes is better than focusing on the outcomes alone[x].
Reporting on a wide range of OSH statistics via Corporate Sustainability Reporting (CSR) to investors helps to maintain a senior management and executive focus on reducing injuries[xi].
Lessons Learned
Reflecting on possible underlying causes of the SIF problem while writing various OSH texts over the past 3 years led to a sudden and surprising understanding: the global OSH profession has been focusing upon ‘epiphenomena’ that have no causal relationships to SIFs. It has been trying to address the incidental byproduct(s) of various work-related activities (e.g., stress), rather than tangible SIF precursor situations (e.g., unexpected maintenance), exposure categories (e.g., confined space entry) and underlying contributors (e.g., inadequate job methods).
With an escalating global problem, the OSH profession needs to adopt and pursue a laser-like focus on preventing SIFs. There are known evidence-based solutions which have been available for decades; for some unknown reason, a large portion of the OSH profession appears to take them for granted and/or has turned its back on them. Continuing to focus on epiphenomena means the SIF problem will only get much worse.
Where the leadership is going to come from to systematically tackle this global SIF problem (the ILO, national regulators, multinationals, professional OSH bodies or individual OSH professionals) is a genuine concern. Clearly, an adult conversation on the issue is long overdue.
References
[i] ILO. (2017). Snapshots on occupational safety and health (OSH) at the world congress on safety and health at work 2017.
[ii] World Health Organization. (2021). WHO/ILO joint estimates of the work-related burden of disease and injury, 2000–2016: global monitoring report.
[iii] Davies, R., Jones, P., & Nuñez, I. (2009). The impact of the business cycle on occupational injuries in the UK. Social Science & Medicine, 69(2), 178-182.
[iv] Cooper, M. D. (2022). The emperor has no clothes: A critique of Safety-II. Safety Science, 152, 105047.
[v] Cooper, M. D., Collins, M., Bernard, R., Schwann, S., & Knox, R. J. (2019). Criterion-related validity of the cultural web when assessing safety culture. Safety Science, 111, 49-66.
[vi] Cooper, M. D. (2017). Practical steps to reduce Serious Injuries & Fatalities (SIFs). Coalition for Construction Safety Roundtable, Bowen Engineering, Indianapolis, 17 Aug.
[vii] Li, H., Lu, M., Hsu, S. C., Gray, M., & Huang, T. (2015). Proactive behavior-based safety management for construction safety improvement. Safety Science, 75, 107-117.
[viii] Cannon, L. (2012). Alcoa and the human performance journey. In: Gulf Aluminium Council Safety Conference 2012, Gulf Hotel, Bahrain, 12–14th Nov
[ix] Chevron. (2012). Operational Excellence at Chevron.
[x] Health & Safety Executive (2001). A guide to measuring health & safety performance. HSE Books.
[xi] Cooper, M. D. (2019). The efficacy of industrial safety science constructs for addressing serious injuries & fatalities (SIFs). Safety Science, 120, 164-178.
Approaches to managing the risks associated Musculoskeletal disorders
In this episode of the Safety & Health Podcast, we hear from Matt Birtles, Principal Ergonomics Consultant at HSE’s Science and Research Centre, about the different approaches to managing the risks associated with Musculoskeletal disorders.
Matt, an ergonomics and human factors expert, shares his thoughts on why MSDs are important, the various prevalent rates across the UK, what you can do within your own organisation and the Risk Management process surrounding MSD’s.

Thanks Dom. Great read.
Thanks for this interesting and thought provoking article.
In my opinion, the epiphenomena mentioned in the article, contribute directly to the formation of people’s attitudes towards their own physical (and psychological) health and safety.
Therefore a combined approach i.e. assessing the effective of the epiphenomena in achieving improvement (i.e. less SIF’s), coupled with robust adherence to the hierarch of controls, offers a reasonable chance of achieving the best possible outcomes.
This was a brilliant Article. Thanks Dr Cooper. I think what is also clear for me is every level of an organization has a role to play in reducing SIF’s. From Executive levels, Shareholders, Senior Management, middle Management and blue collar personnel all have different roles to play. They should all ally the various strategies and ensure its being done, effectively and monitored to for continuous improvement.
Thanks again.
Hi Dom, Some of your global stats are out of date and this undermines your premise. The data sources and methods used to estimate the work-related deaths may vary by year and country. The WHO and ILO report you quoted provides more comprehensive and consistent estimates of the global and regional trends over time. According to the WHO/ILO joint report, the global number of work-related deaths from injuries decreased by 14.6% from 2000 to 2016. The report estimates that there were 399 000 work-related deaths from injuries in 2000, and 341 000 in 2016. The report also shows that the global… Read more »
Think this one has been discussed to death (excuse the pun) on LinkedIn. There are many different reports by different people. I could not find where the WHO/ILO report dismisses the 1999 1million estimate. The 2000 Chinese data of 20K in this WHO/ILO joint report differs hugely from to 78k in 1998 & 90k in 2001 reported in the scientific journals that estimated 2.3 million SIFs in 2003. Thus, different reports produce different results.The main takeaway is there are far too many SIFs and the problem is growing. Equally, epiphenomena won’t fix the problem simply by virtue of them being… Read more »
Absolutely agree with this approach, its a pity more people are not signed up to this approach